NYC's Premier Physical Therapy and Rehabilitation Clinic
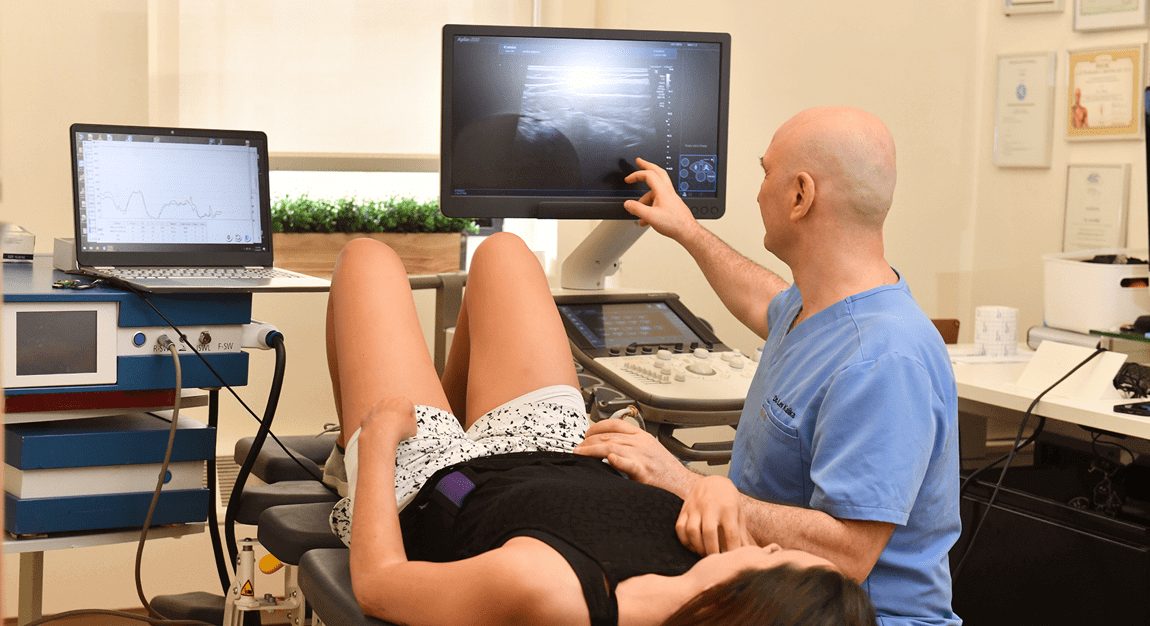
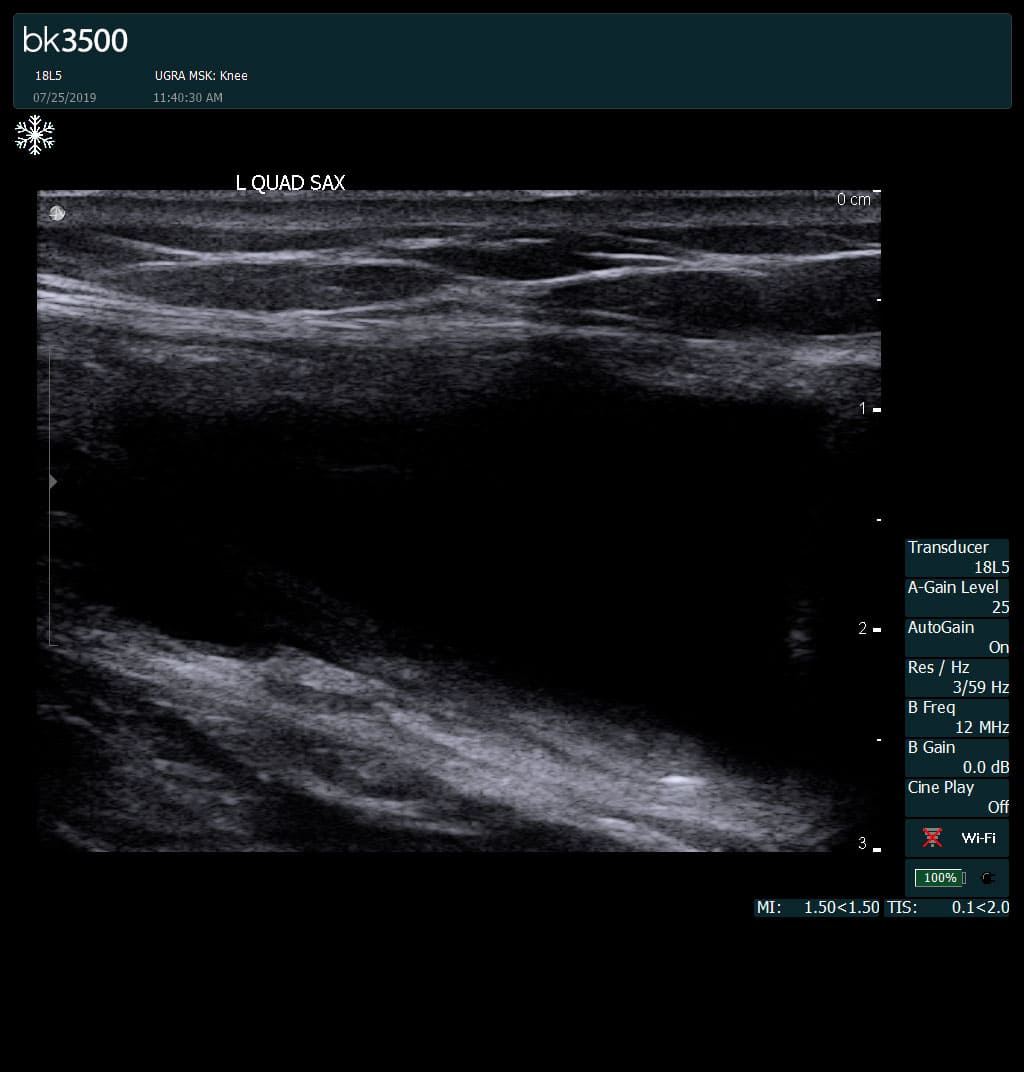
NYDNRehab’s team of sports physical therapists and chiropractors leverage the most advanced technologies to provide our patients with the best evidence-based therapeutic treatment options. Our research-grade motion analysis technology and high resolution diagnostic ultrasonography help us to accurately detect motor deviations that are invisible to the human eye. Our personalized treatment plans are data-driven. We quantify your progress step-by-step, until your goals are reached and pain-free movement is restored. Our unique approach to personalized one-on-one patient care makes NYDNRehab the premier clinic for physical therapy and injury rehabilitation in Midtown Manhattan. We are recognized experts in the field of physical therapy and rehabilitative medicine. We have been chosen as a Top-20 physical therapy clinic by expertise.com for the 5th year in the row…
Certifications


![]()